Helpful resources for you and your patients with RA
Resources for healthcare providers



Medication Guide/Instructions for Use
.png/jcr:content/Monotherapy%20Brochure%20Thumbnail%20(1).png 400w, /.imaging/webp/sanofi-platform/img-w500/dam/kevzara-ra-com-hcp/resources/Monotherapy-Brochure-Thumbnail-(1).png/jcr:content/Monotherapy%20Brochure%20Thumbnail%20(1).png 500w)
Monotherapy Reprint Carrier
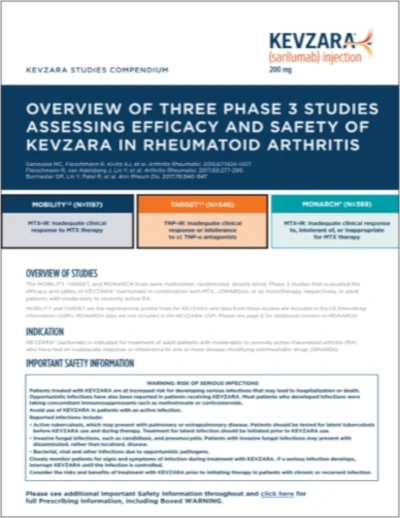
Three Studies Compendium
KevzaraConnect® tools

-Application-Digital.png/jcr:content/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png 400w, /.imaging/webp/sanofi-platform/img-w500/dam/kevzara-ra-com-hcp/resources-and-financial-support/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png/jcr:content/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png 500w, /.imaging/webp/sanofi-platform/img-w600/dam/kevzara-ra-com-hcp/resources-and-financial-support/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png/jcr:content/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png 600w, /.imaging/webp/sanofi-platform/img-w700/dam/kevzara-ra-com-hcp/resources-and-financial-support/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png/jcr:content/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png 700w, /.imaging/webp/sanofi-platform/img-w800/dam/kevzara-ra-com-hcp/resources-and-financial-support/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png/jcr:content/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png 800w, /.imaging/webp/sanofi-platform/img-w900/dam/kevzara-ra-com-hcp/resources-and-financial-support/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png/jcr:content/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png 900w, /.imaging/webp/sanofi-platform/img-w1200/dam/kevzara-ra-com-hcp/resources-and-financial-support/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png/jcr:content/KevzaraConnect-Patient-Assistance-Program-(PAP)-Application-Digital.png 1200w)
Patient Assistance Program Application

Sample Letter Template: Appeals

Sample Letter Template: Medical Necessity

KEVZARA sample letters are included to help provide the type of information that may be useful when responding to a health plan. These letters provide an example of the types of information that may be provided when responding to a request from a patient’s health plan to provide either a letter of appeal or a letter of medical necessity for KEVZARA. Use of the information in these letters does not guarantee that the health plan will cover KEVZARA and is not intended to be a substitute for or an influence on the independent medical judgment of the physician.
Watch Educational Videos
Watch how KEVZARA helps inhibit IL-6–related RA disease activity.
- adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs (DMARDs).
- adult patients with polymyalgia rheumatica (PMR) who have had an inadequate response to corticosteroids or who cannot tolerate corticosteroid taper.
- Active tuberculosis, which may present with pulmonary or extrapulmonary disease. Patients should be tested for latent tuberculosis before KEVZARA use and during therapy. Treatment for latent infection should be initiated prior to KEVZARA use.
- Invasive fungal infections, such as candidiasis, and pneumocystis. Patients with invasive fungal infections may present with disseminated, rather than localized, disease.
- Bacterial, viral and other infections due to opportunistic pathogens.
- Infections. Serious and sometimes fatal infections due to bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens have been reported in patients receiving immunosuppressive agents including KEVZARA. Among opportunistic infections, TB, candidiasis, and pneumocystis were reported with KEVZARA. The most frequently observed serious infections with KEVZARA in RA patients included pneumonia and cellulitis.
- Hold treatment with KEVZARA if a patient develops a serious infection or an opportunistic infection.
- Patients with latent TB should be treated with standard antimycobacterial therapy before initiating KEVZARA. Consider anti-TB therapy prior to initiation of KEVZARA in patients with a past history of latent or active TB in whom an adequate course of treatment cannot be confirmed, and for patients with a negative test for latent TB but having risk factors for TB infection.
- Consider the risks and benefits of treatment prior to initiating KEVZARA in patients who have: chronic or recurrent infection, a history of serious or opportunistic infections, underlying conditions that may predispose them to infection, been exposed to TB, or lived in or traveled to areas of endemic TB or endemic mycoses.
- Viral reactivation has been reported with immunosuppressive biologic therapies. Cases of herpes zoster were observed in clinical studies with KEVZARA.
- Laboratory Abnormalities. Treatment with KEVZARA was associated with decreases in absolute neutrophil counts (including neutropenia), and platelet counts; and increases in transaminase levels and lipid parameters (LDL, HDL cholesterol, and/or triglycerides). Increased frequency and magnitude of these elevations were observed when potentially hepatotoxic drugs (e.g., MTX) were used in combination with KEVZARA. Assess neutrophil count, platelet count, and ALT/AST levels prior to initiation with KEVZARA. Monitor these parameters 4 to 8 weeks after start of therapy and every 3 months thereafter. Assess lipid parameters 4 to 8 weeks after start of therapy, then at 6 month intervals.
- Gastrointestinal Perforation. GI perforation risk may be increased with concurrent diverticulitis or concomitant use of NSAIDs or corticosteroids. Gastrointestinal perforations have been reported in clinical studies, primarily as complications of diverticulitis. Promptly evaluate patients presenting with new onset abdominal symptoms.
- Immunosuppression. Treatment with immunosuppressants may result in an increased risk of malignancies. The impact of treatment with KEVZARA on the development of malignancies is not known but malignancies have been reported in clinical studies.
- Hypersensitivity Reactions. Hypersensitivity reactions have been reported in association with KEVZARA. Hypersensitivity reactions that required treatment discontinuation were reported in 0.3% of patients in controlled RA trials. Injection site rash, rash, and urticaria were the most frequent hypersensitivity reactions. Advise patients to seek immediate medical attention if they experience any symptoms of a hypersensitivity reaction. If anaphylaxis or other hypersensitivity reaction occurs, stop administration of KEVZARA immediately. Do not administer KEVZARA to patients with known hypersensitivity to sarilumab.
- Active Hepatic Disease and Hepatic Impairment. Treatment with KEVZARA is not recommended in patients with active hepatic disease or hepatic impairment, as treatment with KEVZARA was associated with transaminase elevations.
- Live Vaccines. Avoid concurrent use of live vaccines during treatment with KEVZARA due to potentially increased risk of infections. No data are available on the secondary transmission of infection from persons receiving live vaccines to patients receiving KEVZARA. Prior to initiating treatment, it is recommended that all patients be brought up to date with all immunizations in agreement with current immunization guidelines.
- For Rheumatoid Arthritis: The most common serious adverse reactions were infections. The most frequently observed serious infections included pneumonia and cellulitis. The most common adverse reactions (occurred in at least 3% of patients treated with KEVZARA + DMARDs) are neutropenia, increased ALT, injection site erythema, upper respiratory infections, and urinary tract infections.
- For Polymyalgia Rheumatica: Serious adverse reactions of neutropenia occurred in 2 patients (3.4%) in the KEVZARA group compared to none in the placebo group. The proportion of patients with serious infections was similar in the KEVZARA group (5.1%) compared to the placebo group (5.2%). The common adverse reactions occurring in ≥5% of patients treated with KEVZARA were neutropenia, leukopenia, constipation, rash pruritic, myalgia, fatigue, and injection site pruritus.
- Exercise caution when KEVZARA is co-administered with CYP substrates with a narrow therapeutic index (e.g. warfarin or theophylline), or with CYP3A4 substrates (e.g. oral contraceptives or statins) as there may be a reduction in exposure which may reduce the activity of the CYP3A4 substrate.
- Elevated interleukin-6 (IL-6) concentration may down-regulate CYP activity such as in patients with RA and hence increase drug levels compared to subjects without RA. Blockade of IL-6 signaling by IL-6Rα antagonists such as KEVZARA might reverse the inhibitory effect of IL-6 and restore CYP activity, leading to altered drug concentrations.
- KEVZARA should be used in pregnancy only if the potential benefit justifies the potential risk to the fetus. Because monoclonal antibodies could be excreted in small amounts in human milk, the benefits of breastfeeding and the potential adverse effects on the breastfed child should be considered along with the mother’s clinical need for KEVZARA.
- Use caution when treating the elderly.
TRANSCRIPT
Inflammatory rheumatic diseases like rheumatoid arthritis, or RA, and polymyalgia rheumatica, or PMR, are systemic autoimmune diseases characterized by persistent inflammation1-3 which can lead to impaired joint and muscle function, pain, and difficulty performing daily routines.1,4,5
Pro-inflammatory cytokines, such as Interleukin-6, or IL-6, immune cells, such as T cells and macrophages, tumor necrosis factor alpha, or TNF-alpha, as well as intracellular signaling pathways, such as Janus kinase and signal transducer and activator of transcription, or JAK/STAT, contribute to disease development and progression.6-12
IL-6 serum levels in particular are elevated in patients with inflammatory rheumatic diseases. They play a central role in the inflammatory pathways that may lead to chronic inflammation, morning stiffness, and systemic manifestations, including pain, and in the case of RA, disease progression.5,6,13-17
IL-6 is a key cytokine featuring pleiotropic activity. The effects of IL-6 include stimulation of acute phase protein synthesis, such as C-reactive protein, or CRP, serum amyloid A, fibrinogen, and induced hepcidin production by hepatocytes. IL-6 also inhibits the production of albumin. IL-6 plays an important role in immune response by stimulating antibody-producing B cells and influencing effector T-cell development. Dysregulated, continuous IL-6 production may be associated with the development of inflammatory autoimmune diseases.6,11,14,18
IL-6 exerts its inflammatory effects through activation of certain proinflammatory signaling pathways important to inflammatory rheumatic diseases.7
IL-6 primarily activates the JAK/STAT pathway, as well as the mitogen-activated protein kinase, or MAPK, signaling pathway, and the phosphoinositide 3-kinase, or PI3K, signaling pathway.6,19-22
These signaling features help explain both the overlapping and distinct roles that IL-6 and JAK/STAT play in the pathogenesis of inflammatory rheumatic diseases.7,19
Persistently elevated levels of IL-6 are a major driver of inflammation in RA and PMR.4,11,13,14,18,23,24
While several cytokines signal only through membrane-bound receptors, IL-6 acts through a dual signaling mechanism involving both a soluble and cell membrane-bound receptors.6
The IL-6/IL-6 receptor complexes become activated when they associate with glycoprotein 130, or gp130, a transmembrane receptor expressed in abundance on the surface of most cells.5,25,26
As a result, elevated levels of IL-6 have widespread effects throughout the body, modulating both adaptive and innate immune responses.7,27
It is also important to note that systemic inflammation can be associated with activation of an acute phase response, like CRP.7,11,28
The ability to modulate these effects may be important to control disease activity.7,11,23
KEVZARA, or sarilumab, is the only fully human monoclonal antibody that inhibits IL-6 receptor signaling.29
KEVZARA targets and binds with high affinity to both soluble and membrane-bound IL-6 receptors, thereby inhibiting IL-6 signaling.29,30
In this way, KEVZARA helps disrupt the effects of elevated IL-6 levels in adult patients with moderately to severely active RA who have had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs, or DMARDs, and adult patients with PMR who have had an inadequate response to corticosteroids or who cannot tolerate corticosteroid taper.29
Thank you for watching.
INDICATIONS
KEVZARA® (sarilumab) is indicated for treatment of:
IMPORTANT SAFETY INFORMATION
WARNING: RISK OF SERIOUS INFECTIONS
Patients treated with KEVZARA are at increased risk for developing serious infections that may lead to hospitalization or death. Opportunistic infections have also been reported in patients receiving KEVZARA. Most patients who developed infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids.
Avoid use of KEVZARA in patients with an active infection.
Reported infections include:
Closely monitor patients for signs and symptoms of infection during treatment with KEVZARA. If a serious infection develops, interrupt KEVZARA until the infection is controlled.
Consider the risks and benefits of treatment with KEVZARA prior to initiating therapy in patients with chronic or recurrent infection.
CONTRAINDICATION
Do not use KEVZARA in patients with known hypersensitivity to sarilumab or any of the inactive ingredients.
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
Advise patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Please click here to see full Prescribing Information, including Boxed WARNING.
References: 1. Aletaha D, Neogi T, Silman AT, et al. 2010 Rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569-2581. 2. Bartoloni E, Pucci G, Alunno A, Gerli R, Schillaci G. Polymyalgia rheumatica. In: Nussinovitch U, ed. The Heart in Rheumatic, Autoimmune and Inflammatory Diseases. Academic Press; 2017:213-231. 3. Prior JA, Muller S, Helliwell T, et al. The association of pain and stiffness with fatigue in incident polymyalgia rheumatica: baseline results from the polymyalgia rheumatica cohort study. Prim Health Care Res Dev. 2019;20(e46):1-6. doi:10.1017/S1463423619000082. 4. González-Gay MA, Matteson EL, Castañeda S. Polymyalgia rheumatica. Lancet. 2017;390:1700-1712. 5. Acharya S, Musa R. Polymyalgia Rheumatica. NCBI Bookshelf. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022. 6. Dayer J-M, Choy E. Therapeutic targets in rheumatoid arthritis: the interleukin-6 receptor. Rheumatology (Oxford). 2010;49(1):15-24. 7. Choy E. Understanding the dynamics: pathways involved in the pathogenesis of rheumatoid arthritis. Rheumatology (Oxford). 2012;51(suppl 5):v3-v11. 8. Schwartz DM, Bonelli M, Gadina M, O’Shea JJ. Type I/II cytokines, JAKs, and new strategies for treating autoimmune diseases. Nat Rev Rheumatol. 2016;12(1):25-36. 9. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi: 10.1101/cshperspect.a016295. 10. González-Gay MA, Pina T, Prieto-Peña D, Calderon-Goercke M, Blanco R, Castañeda S. Drug therapies for polymyalgia rheumatica: a pharmacotherapeutic update. Expert Opin Pharmacother. 2018;19(11):1235-1244. 11. Tanaka T, Narazaki M. Interleukin-6 inhibition in inflammatory diseases: results achieved and tasks to accomplish. J Scleroderma Relat Disord. 2017;2(2_suppl):S20-S28. 12. Toussirot E, Régent A, Devauchelle-Pensec V, Saraux A, Puéchal X. Interleukin-6: a promising target for the treatment of polymyalgia rheumatica or giant cell arteritis? RMD Open. 2016;2(2):e000305. doi:10.1136/rmdopen-2016-000305. 13. Jiemy WF, Zhang A, Boots AMH, et al. Expression of interleukin-6 in synovial tissue of patients with polymyalgia rheumatica. Ann Rheum Dis. 2022;0:1-2. doi:10.1136/ard-2022-222873. 14. Alegria GC, Boukhlal S, Cornec D, Devauchelle-Pensec V. The pathophysiology of polymyalgia rheumatica, small pieces of a big puzzle. Autoimmun Rev. 2020;19(11):102670. doi:10.1016/j.autrev.2020.102670. 15. Gibbs JE, Ray DW. The role of the circadian clock in rheumatoid arthritis. Arthritis Res Ther. 2013;15(205):1-10. 16. Grygiel-Górniak B, Puszczewicz M. Fatigue and interleukin-6—a multi-faceted relationship. Reumatologia. 2015;53(4):207-212. 17. Lundberg IE, Sharma A, Turesson C, Mohammed AJ. An update on polymyalgia rheumatica. J Intern Med. 2022;292(5):717-732. 18. Rose-John S, Scheller J, Elson G, Jones SA. Interleukin-6 biology is coordinated by membrane-bound and soluble receptors: role in inflammation and cancer. J Leukoc Biol. 2006;80(2):227-236. 19. Woś I, Tabarkiewicz J. Effect of interleukin-6, -17, -21, -22, and -23 and STAT3 on signal transduction pathways and their inhibition in autoimmune arthritis. Immunol Res. 2021;69(1):26-42. 20. Heinrich PC, Behrmann I, Haan S, Hermanns HM, Müller-Newen G, Schaper F. Principles of interleukin (IL)-6-type cytokine signalling and its regulation. Biochem J. 2003;374(Pt 1):1-20. doi: 10.1042/BJ20030407. 21. Cahill CM, Rogers JT. Interleukin (IL) 1ß induction of IL-6 is mediated by a novel phosphatidylinositol 3-kinase-dependent AKT/IϰB kinase α pathway targeting activator protein-1. J Biol Chem. 2008;283(38):25900-25912. 22. Zegeye MM, Lindkvist M, Fälker K, et al. Activation of the JAK/STAT3 and PI3K/AKT pathways are crucial for IL-6 trans-signaling-mediated pro-inflammatory response in human vascular endothelial cells. Cell Commun Signal. 2018;16(1):55. doi:10.1186/s12964-018-0268-4. 23. Srirangan S, Choy EH. The role of interleukin 6 in the pathophysiology of rheumatoid arthritis. Ther Adv Musculoskelet Dis. 2010;2(5):247-256. 24. Salvarani C, Cantini F, Niccoli L, et al. Acute-phase reactants and the risk of relapse/recurrence in polymyalgia rheumatica: a prospective followup study. Arthritis Rheum. 2005;53(1):33-38. 25. Witte T. Methotrexate as combination partner of TNF inhibitors and tocilizumab. What is reasonable from an immunological viewpoint? Clin Rheumatol. 2015;34(4):629-634. doi:10.1007/s10067-015-2861-x. 26. Boettger MK, Leuchtweis J, Kümmel D, Gajda M, Braüer R, Schaible H-G. Differential effects of locally and systemically administered soluble glycoprotein 130 on pain and inflammation in experimental arthritis. Arthritis Res Ther. 2010;12(4):R140. doi:10.1186/ar3079. 27. Gierut A, Perlman H, Pope RM. Innate immunity and rheumatoid arthritis. Rheum Dis Clin North Am. 2010;36(2):271-296. 28. Black AP, Bhayani H, Ryder CA, Pugh MT, Gardner-Medwin JM, Southwood TR. An association between the acute phase response and patterns of antigen induced T cell proliferation in juvenile idiopathic arthritis. Arthritis Res Ther. 2003;5(5):R277-R284. doi:10.1186/ar791. 29. KEVZARA [prescribing information]. Bridgewater, NJ: Sanofi/Regeneron Pharmaceuticals, Inc. 30. Genovese MC, Fleischmann R, Kivitz AJ, et al. Sarilumab plus methotrexate in patients with active rheumatoid arthritis and inadequate response to methotrexate: results of a phase III study. Arthritis Rheumatol. 2015;67(6):1424-1437.
Watch Ms Audrey Gibson share her clinical expertise, discussing combination trial data for KEVZARA.
- Active tuberculosis, which may present with pulmonary or extrapulmonary disease. Patients should be tested for latent tuberculosis before KEVZARA use and during therapy. Treatment for latent infection should be initiated prior to KEVZARA use.
- Invasive fungal infections, such as candidiasis, and pneumocystis. Patients with invasive fungal infections may present with disseminated, rather than localized, disease.
- Bacterial, viral and other infections due to opportunistic pathogens.
- Infections. Serious and sometimes fatal infections due to bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens have been reported in patients receiving immunosuppressive agents including KEVZARA. Among opportunistic infections, TB, candidiasis, and pneumocystis were reported with KEVZARA. The most frequently observed serious infections with KEVZARA in RA patients included pneumonia and cellulitis.
- Hold treatment with KEVZARA if a patient develops a serious infection or an opportunistic infection.
- Patients with latent TB should be treated with standard antimycobacterial therapy before initiating KEVZARA. Consider anti-TB therapy prior to initiation of KEVZARA in patients with a past history of latent or active TB in whom an adequate course of treatment cannot be confirmed, and for patients with a negative test for latent TB but having risk factors for TB infection.
- Consider the risks and benefits of treatment prior to initiating KEVZARA in patients who have: chronic or recurrent infection, a history of serious or opportunistic infections, underlying conditions that may predispose them to infection, been exposed to TB, or lived in or traveled to areas of endemic TB or endemic mycoses.
- Viral reactivation has been reported with immunosuppressive biologic therapies. Cases of herpes zoster were observed in clinical studies with KEVZARA.
- Laboratory Abnormalities. Treatment with KEVZARA was associated with decreases in absolute neutrophil counts (including neutropenia), and platelet counts; and increases in transaminase levels and lipid parameters (LDL, HDL cholesterol, and/or triglycerides). Increased frequency and magnitude of these elevations were observed when potentially hepatotoxic drugs (e.g., MTX) were used in combination with KEVZARA. Assess neutrophil count, platelet count, and ALT/AST levels prior to initiation with KEVZARA. Monitor these parameters 4 to 8 weeks after start of therapy and every 3 months thereafter. Assess lipid parameters 4 to 8 weeks after start of therapy, then at 6 month intervals.
- Gastrointestinal Perforation. GI perforation risk may be increased with concurrent diverticulitis or concomitant use of NSAIDs or corticosteroids. Gastrointestinal perforations have been reported in clinical studies, primarily as complications of diverticulitis. Promptly evaluate patients presenting with new onset abdominal symptoms.
- Immunosuppression. Treatment with immunosuppressants may result in an increased risk of malignancies. The impact of treatment with KEVZARA on the development of malignancies is not known but malignancies have been reported in clinical studies.
- Hypersensitivity Reactions. Hypersensitivity reactions have been reported in association with KEVZARA. Hypersensitivity reactions that required treatment discontinuation were reported in 0.3% of patients in controlled RA trials. Injection site rash, rash, and urticaria were the most frequent hypersensitivity reactions. Advise patients to seek immediate medical attention if they experience any symptoms of a hypersensitivity reaction. If anaphylaxis or other hypersensitivity reaction occurs, stop administration of KEVZARA immediately. Do not administer KEVZARA to patients with known hypersensitivity to sarilumab.
- Active Hepatic Disease and Hepatic Impairment. Treatment with KEVZARA is not recommended in patients with active hepatic disease or hepatic impairment, as treatment with KEVZARA was associated with transaminase elevations.
- Live Vaccines. Avoid concurrent use of live vaccines during treatment with KEVZARA due to potentially increased risk of infections. No data are available on the secondary transmission of infection from persons receiving live vaccines to patients receiving KEVZARA. Prior to initiating treatment, it is recommended that all patients be brought up to date with all immunizations in agreement with current immunization guidelines.
- For Rheumatoid Arthritis: The most common serious adverse reactions were infections. The most frequently observed serious infections included pneumonia and cellulitis. The most common adverse reactions (occurred in at least 3% of patients treated with KEVZARA + DMARDs) are neutropenia, increased ALT, injection site erythema, upper respiratory infections, and urinary tract infections.
- Exercise caution when KEVZARA is co-administered with CYP substrates with a narrow therapeutic index (e.g. warfarin or theophylline), or with CYP3A4 substrates (e.g. oral contraceptives or statins) as there may be a reduction in exposure which may reduce the activity of the CYP3A4 substrate.
- Elevated interleukin-6 (IL-6) concentration may down-regulate CYP activity such as in patients with RA and hence increase drug levels compared to subjects without RA. Blockade of IL-6 signaling by IL-6Rα antagonists such as KEVZARA might reverse the inhibitory effect of IL-6 and restore CYP activity, leading to altered drug concentrations.
- KEVZARA should be used in pregnancy only if the potential benefit justifies the potential risk to the fetus. Because monoclonal antibodies could be excreted in small amounts in human milk, the benefits of breastfeeding and the potential adverse effects on the breastfed child should be considered along with the mother’s clinical need for KEVZARA.
- Use caution when treating the elderly.
TRANSCRIPT
[Introduction. 00:00-00:11]
Hello, my name is Audrey Gibson and I’m a physician assistant at the Arthritis Center of North Georgia.
I’m excited to share some information with you about KEVZARA in combination therapy.
[KEVZARA Indication and Boxed Warning. 00:11-00:44]
KEVZARA is indicated for treatment of adult patients with moderately to severely active rheumatoid arthritis, who have an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs. Patients treated with KEVZARA are at an increased risk for developing serious infections that may lead to hospitalization or death. Avoid use of KEVZARA in patients with an active infection and closely monitor patients for signs and symptoms of infection during treatment with KEVZARA. This will be discussed more, along with additional important safety information, later in this video.1
[Factors that influence decision to prescribe concomitant therapy. 00:44-01:14]
“When considering a concomitant therapy, what factors influence your decision on what to prescribe?”
When considering a concomitant therapy for my RA patients, first I look closely at the clinical trial data. For KEVZARA, the trials that are most important to me in this context are MOBILITY, which evaluated the methotrexate inadequate responder population; TARGET, which evaluated TNF inadequate responder patients; and EXTEND, which is a long-term extension study of KEVZARA in combination with methotrexate or other DMARDs.1,2
[MOBILITY trial study design. 01:14-01:46]
First let’s look at MOBILITY. MOBILITY was a 52-week, randomized, double-blind, placebo-controlled, multi-center study, which included 1,197 patients. It assessed the efficacy and safety of KEVZARA 200 milligrams plus methotrexate, and 150 milligrams plus methotrexate, in patients with moderate to severe active rheumatoid arthritis, with a duration of at least three months, who had been on methotrexate 10 milligrams to 25 milligrams per week for at least six weeks.1,3
[TARGET trial study design. 01:46-02:20]
Next, let’s look at TARGET. TARGET was a 24-week randomized, double-blind parallel group, placebo-controlled, multi-center study, which included 546 patients. It assessed the efficacy and safety of KEVZARA 200 milligrams, and 150 milligrams added to background conventional DMARDs in patients with moderate to severe active rheumatoid arthritis, with a duration of at least six months, with inadequate response and/or intolerance to one or more TNF antagonists, when administered with background conventional DMARDs.1,4
[MOBILITY and TARGET patients enrolled. 02:20-02:45]
The patient population of both MOBILITY and TARGET are relevant as it is representative of the types of patients that I see in my practice. These are patients that have failed both methotrexate and one or more TNFs.
When I look at the data, it is notable that, in all three study arms for TARGET, over 20 percent of patients had cycled through multiple TNFs. And so that gives me confidence that these trials are characteristic of what I see in my patients in real life.4
[MOBILITY and TARGET coprimary endpoints. 02:45-03:05]
Let’s take a look at the co-primary endpoints. The co-primary endpoints evaluated were the proportion of patients who achieved an ACR20 response at week 24, the change from baseline in HAQ-DI at week 16 in MOBILITY and week 12 in TARGET, and the change from baseline in mean Total Sharp Score at week 52 in MOBILITY.1
[MOBILITY and TARGET efficacy data. 03:05-04:40]
Now let’s take a look at the outcomes. As you can see, there were consistent results across both trials.
Looking at MOBILITY, significantly more patients in the KEVZARA 200 milligram plus methotrexate group achieved an ACR20 response at 24 weeks, compared to placebo plus methotrexate group: 66 percent versus 33 percent, respectively.1,3
Now, let’s look at TARGET. Significantly more patients in the KEVZARA 200 milligram plus DMARD group achieved an ACR20 response at 24 weeks than in the placebo plus DMARD group: 61 percent versus 34 percent, respectively. Now, keep in mind that these are patients that have failed one or more TNFs.1,4
I’m excited about the consistency across trials, because I find replication of results is the hallmark of scientific rigor. And it helps me feel that I am making more informed decisions when prescribing.
Other information that I found interesting was that the third co-primary endpoint in the MOBILITY trial, was change from baseline in mean Total Sharp Scores at 52 weeks. Both doses of KEVZARA plus methotrexate were associated with significantly less radiographic progression of structural damage compared with placebo plus methotrexate at 52 weeks. Improvements were also observed with both doses of KEVZARA at 24 weeks.1,3
More than half of patients—55.6 percent—receiving KEVZARA 200 milligrams plus methotrexate, had no evidence of any radiographic progression at 52 weeks, compared with 38.7 percent of patients receiving placebo plus methotrexate.3
[MOBILITY and TARGET safety data. 04:40-05:03]
Next, let’s look at some of the safety data. In here, you can see the most common adverse reactions in the trials: neutropenia, increased ALT, and injection site erythema. For the most frequent adverse events, KEVZARA demonstrated 10 percent, five percent, and four percent versus 0.2 percent, two percent, and 0.9 percent with placebo.1
[Consider KEVZARA for your patients with RA. 05:03-05:54]
When talking to a patient, and I can tell that they’re not doing well, this is when I discuss making a change in their medication.
I consider combination therapy in any patient who is not doing well on their current drug regimen—any patient that is having persistent joint pain, or swelling, or having more flares.
I suggest that it may be time for a change.
I have chosen KEVZARA as a treatment when patients have failed both methotrexate and TNFs. I have made this decision based off data from both the MOBILITY and the TARGET trials.1
There is more information available that can help you better understand the long-term efficacy and safety of KEVZARA. Although not a focus of this video, I encourage you to look at the Open Label Extension trial EXTEND, which followed patients out to seven years. This data is available on combination therapy page on this website.
INDICATION
KEVZARA® (sarilumab) is indicated for treatment of adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs (DMARDs).
IMPORTANT SAFETY INFORMATION
WARNING: RISK OF SERIOUS INFECTIONS
Patients treated with KEVZARA are at increased risk for developing serious infections that may lead to hospitalization or death. Opportunistic infections have also been reported in patients receiving KEVZARA. Most patients who developed infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids.
Avoid use of KEVZARA in patients with an active infection.
Reported infections include:
Closely monitor patients for signs and symptoms of infection during treatment with KEVZARA. If a serious infection develops, interrupt KEVZARA until the infection is controlled.
Consider the risks and benefits of treatment with KEVZARA prior to initiating therapy in patients with chronic or recurrent infection.
CONTRAINDICATION
Do not use KEVZARA in patients with known hypersensitivity to sarilumab or any of the inactive ingredients.
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
Advise patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Please click here to see full Prescribing Information, including Boxed WARNING.
References: 1. Kevzara [prescribing information]. Bridgewater, NJ: Sanofi/Regeneron Pharmaceuticals, Inc. 2. Data on file. Bridgewater, NJ: Sanofi/Regeneron. EXTEND Clinical Study Report. January 2016. 3. Genovese MC, Fleischmann R, Kivitz AJ, et al. Sarilumab plus methotrexate in patients with active rheumatoid arthritis and inadequate response to methotrexate. Arthritis Rheumatol. 2015;67(6):1424-1437. 4. Fleischmann R, Adelsberg JV, Lin Y, et al. Sarilumab and nonbiologic disease-modifying antirheumatic drugs in patients with active rheumatoid arthritis and inadequate response or intolerance to tumor necrosis factor inhibitors. Arthritis Rheumatol. 2017;69(2):277-290.
Watch Dr Suzanne Gharib share her clinical expertise, discussing the importance of head-to-head monotherapy data for KEVZARA.
- Active tuberculosis, which may present with pulmonary or extrapulmonary disease. Patients should be tested for latent tuberculosis before KEVZARA use and during therapy. Treatment for latent infection should be initiated prior to KEVZARA use.
- Invasive fungal infections, such as candidiasis, and pneumocystis. Patients with invasive fungal infections may present with disseminated, rather than localized, disease.
- Bacterial, viral and other infections due to opportunistic pathogens.
- Infections. Serious and sometimes fatal infections due to bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens have been reported in patients receiving immunosuppressive agents including KEVZARA. Among opportunistic infections, TB, candidiasis, and pneumocystis were reported with KEVZARA. The most frequently observed serious infections with KEVZARA in RA patients included pneumonia and cellulitis.
- Hold treatment with KEVZARA if a patient develops a serious infection or an opportunistic infection.
- Patients with latent TB should be treated with standard antimycobacterial therapy before initiating KEVZARA. Consider anti-TB therapy prior to initiation of KEVZARA in patients with a past history of latent or active TB in whom an adequate course of treatment cannot be confirmed, and for patients with a negative test for latent TB but having risk factors for TB infection.
- Consider the risks and benefits of treatment prior to initiating KEVZARA in patients who have: chronic or recurrent infection, a history of serious or opportunistic infections, underlying conditions that may predispose them to infection, been exposed to TB, or lived in or traveled to areas of endemic TB or endemic mycoses.
- Viral reactivation has been reported with immunosuppressive biologic therapies. Cases of herpes zoster were observed in clinical studies with KEVZARA.
- Laboratory Abnormalities. Treatment with KEVZARA was associated with decreases in absolute neutrophil counts (including neutropenia), and platelet counts; and increases in transaminase levels and lipid parameters (LDL, HDL cholesterol, and/or triglycerides). Increased frequency and magnitude of these elevations were observed when potentially hepatotoxic drugs (e.g., MTX) were used in combination with KEVZARA. Assess neutrophil count, platelet count, and ALT/AST levels prior to initiation with KEVZARA. Monitor these parameters 4 to 8 weeks after start of therapy and every 3 months thereafter. Assess lipid parameters 4 to 8 weeks after start of therapy, then at 6 month intervals.
- Gastrointestinal Perforation. GI perforation risk may be increased with concurrent diverticulitis or concomitant use of NSAIDs or corticosteroids. Gastrointestinal perforations have been reported in clinical studies, primarily as complications of diverticulitis. Promptly evaluate patients presenting with new onset abdominal symptoms.
- Immunosuppression. Treatment with immunosuppressants may result in an increased risk of malignancies. The impact of treatment with KEVZARA on the development of malignancies is not known but malignancies have been reported in clinical studies.
- Hypersensitivity Reactions. Hypersensitivity reactions have been reported in association with KEVZARA. Hypersensitivity reactions that required treatment discontinuation were reported in 0.3% of patients in controlled RA trials. Injection site rash, rash, and urticaria were the most frequent hypersensitivity reactions. Advise patients to seek immediate medical attention if they experience any symptoms of a hypersensitivity reaction. If anaphylaxis or other hypersensitivity reaction occurs, stop administration of KEVZARA immediately. Do not administer KEVZARA to patients with known hypersensitivity to sarilumab.
- Active Hepatic Disease and Hepatic Impairment. Treatment with KEVZARA is not recommended in patients with active hepatic disease or hepatic impairment, as treatment with KEVZARA was associated with transaminase elevations.
- Live Vaccines. Avoid concurrent use of live vaccines during treatment with KEVZARA due to potentially increased risk of infections. No data are available on the secondary transmission of infection from persons receiving live vaccines to patients receiving KEVZARA. Prior to initiating treatment, it is recommended that all patients be brought up to date with all immunizations in agreement with current immunization guidelines.
- For Rheumatoid Arthritis: The most common serious adverse reactions were infections. The most frequently observed serious infections included pneumonia and cellulitis. The most common adverse reactions (occurred in at least 3% of patients treated with KEVZARA + DMARDs) are neutropenia, increased ALT, injection site erythema, upper respiratory infections, and urinary tract infections.
- Exercise caution when KEVZARA is co-administered with CYP substrates with a narrow therapeutic index (e.g. warfarin or theophylline), or with CYP3A4 substrates (e.g. oral contraceptives or statins) as there may be a reduction in exposure which may reduce the activity of the CYP3A4 substrate.
- Elevated interleukin-6 (IL-6) concentration may down-regulate CYP activity such as in patients with RA and hence increase drug levels compared to subjects without RA. Blockade of IL-6 signaling by IL-6Rα antagonists such as KEVZARA might reverse the inhibitory effect of IL-6 and restore CYP activity, leading to altered drug concentrations.
- KEVZARA should be used in pregnancy only if the potential benefit justifies the potential risk to the fetus. Because monoclonal antibodies could be excreted in small amounts in human milk, the benefits of breastfeeding and the potential adverse effects on the breastfed child should be considered along with the mother’s clinical need for KEVZARA.
- Use caution when treating the elderly.
TRANSCRIPT
[Introduction. 00:00-00:20]
Hi, I’m Suzanne Gharib. I’m a rheumatologist in private practice in South Charleston, West Virginia. I have a special interest in research doing rheumatoid arthritis research on a routine basis, and have a very busy clinical practice, as well as an affiliation with Mon General Hospital in Morgantown, West Virginia.
[Considering monotherapy or switching from MTX. 00:20-01:20]
“What inputs do you leverage when considering monotherapy or switching a patient from methotrexate?”
So, when I see a patient who’s not doing well on methotrexate, and I’m considering either switching them or I have somebody on combination therapy, and I’m considering dropping the methotrexate and using the biologic as monotherapy, there’s a few things I consider. One of them is the head-to-head trial data. I think that really helps to guide treatment decisions in rheumatoid arthritis.
Now we, as rheumatologists, tend to ask for head-to-head trials. But we don’t always rely on the information as much as we ought to. I think it’s incredibly important that we review the available clinical trial data, especially if we are considering monotherapy options. So you really need to see the head-to-head results and particularly superiority data.
And one example of that is the MONARCH Trial, which has good data and a head-to-head type setting. And it’s important superiority data.1
[KEVZARA Indication and Safety. 01:20-01:54]
KEVZARA is indicated for the treatment of adult patients with moderately to severely active rheumatoid arthritis, who’ve had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs. Patients treated with KEVZARA are at an increased risk for developing serious infections that may lead to hospitalization or death. Avoid the use of KEVZARA in patients with an active infection, and closely monitor patients for signs and symptoms of infection during treatment with KEVZARA. This will be discussed more, along with additional important safety information, later in the video.2
[Therapeutic optimization for patients with RA. 01:54-02:39]
So, I think if you asked the average rheumatologist, “How many patients are on monotherapy?” they would guess one out of three. I would have said the same, until I saw some recent claims data that says it’s closer to 47 percent.
I believe we have this perception of, “oh patients take exactly what we tell them to take.” And that’s just not reality. What we find on claims data is about half of biologic or synthetic DMARD prescriptions are, in fact, for monotherapy. And the reasons for that are varied. But many patients are either unable or unwilling to use methotrexate for a variety of reasons. So as a healthcare provider, it’s important to select a treatment option that has strong results as both combination therapy, or monotherapy, in the event that patients don’t take their methotrexate.
[Therapeutic changes for patients with RA. 02:39-03:21]
So, when we start patients on methotrexate, do we ever wonder how quickly or how often do they switch—or even another biologic, how quickly do they switch? There’s a lot of data about that. And the looks of it is about half of patients who are initially prescribed methotrexate alone will either switch to a biologic, or add a biologic within a year. Unfortunately, if you follow this graphic, that switch happens recurrently.3,4
That is not necessarily the best thing for the patient. It really highlights the importance of choosing the appropriate therapy, for the appropriate patients, in the appropriate time. And that is really getting to know your patient, their comorbidities, and determining the best agent on that basis.
[Experience treating patients with RA. 03:21-04:15]
When it comes to my patients, I have quite a few on monotherapy. I would say anywhere from 30 to 50 percent. And what drives that is my usual goal is actually to get patients to monotherapy if at all possible. And most patients do not want to take multiple medications.
When I’m prescribing a new therapy, I think it’s incredibly important to consider, not just in the moment, but down the line, can patients move to monotherapy rather than combination therapy?
Traditionally, in RA, we use combination therapy. But we know the data is what the data is. Patients frequently skip medications, will choose to take one or the other. So, it’s incredibly important that when we choose a new biologic or small molecule, that we choose something that has strong results and good delivery as a monotherapy. That gives patients that option in the future.1
[Considering KEVZARA for monotherapy. 04:15-04:46]
When I have a patient who’s not tolerating methotrexate, or has concerns and doesn’t want to take it, and I’m considering monotherapy, one of the biologics I consider strongly is KEVZARA.2
KEVZARA gives strong results versus adalimumab in the MONARCH Trial, making it a good option for my patients interested in monotherapy.1
You can find detailed information about the clinical trial program for KEVZARA, including MONARCH, on the head-to-head monotherapy page of this website.
Please see the following Important Safety Information.
INDICATION
KEVZARA® (sarilumab) is indicated for treatment of adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs (DMARDs).
IMPORTANT SAFETY INFORMATION
WARNING: RISK OF SERIOUS INFECTIONS
Patients treated with KEVZARA are at increased risk for developing serious infections that may lead to hospitalization or death. Opportunistic infections have also been reported in patients receiving KEVZARA. Most patients who developed infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids.
Avoid use of KEVZARA in patients with an active infection.
Reported infections include:
Closely monitor patients for signs and symptoms of infection during treatment with KEVZARA. If a serious infection develops, interrupt KEVZARA until the infection is controlled.
Consider the risks and benefits of treatment with KEVZARA prior to initiating therapy in patients with chronic or recurrent infection.
CONTRAINDICATION
Do not use KEVZARA in patients with known hypersensitivity to sarilumab or any of the inactive ingredients.
WARNINGS AND PRECAUTIONS
ADVERSE REACTIONS
DRUG INTERACTIONS
USE IN SPECIFIC POPULATIONS
Advise patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Please click here to see full Prescribing Information, including Boxed WARNING.
References: 1. Burmester GR, Lin Y, Patel R, et al. Efficacy and safety of sarilumab monotherapy versus adalimumab monotherapy for the treatment of patients with active rheumatoid arthritis (MONARCH): a randomised, double-blind, parallel-group phase III trial. Ann Rheum Dis. 2017;76(5):840-847. 2. Kevzara [prescribing information]. Bridgewater, NJ: Sanofi/Regeneron Pharmaceuticals, Inc. 3. Rohr MK, Mikuls TR, Cohen SB, Thorne CJ, O-Dell JR. The underuse of methotrexate in the treatment of RA: a national analysis of prescribing practices in the U.S. Arthritis Care Res. 2016;69(6):794-800. 4. Fraenkel L, Bathon JM, England BR, et al. 2021 American College of Rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheum. 2021;73(7):1108-1123.
IL-6=interleukin-6; RA=rheumatoid arthritis.
IMPORTANT SAFETY INFORMATION
|
WARNING: RISK OF SERIOUS INFECTIONS Patients treated with KEVZARA are at increased risk for developing serious infections that may lead to hospitalization or death. Opportunistic infections have also been reported in patients receiving KEVZARA. Most patients who developed infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids. Avoid use of KEVZARA in patients with an active infection. Reported infections include:
Closely monitor patients for signs and symptoms of infection during treatment with KEVZARA. If a serious infection develops, interrupt KEVZARA until the infection is controlled. Consider the risks and benefits of treatment with KEVZARA prior to initiating therapy in patients with chronic or recurrent infection. |
CONTRAINDICATION
Do not use KEVZARA in patients with known hypersensitivity to sarilumab or any of the inactive ingredients.
WARNINGS AND PRECAUTIONS
- Infections. Serious and sometimes fatal infections due to bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens have been reported in patients receiving immunosuppressive agents including KEVZARA. Among opportunistic infections, TB, candidiasis, and pneumocystis were reported with KEVZARA. The most frequently observed serious infections with KEVZARA in RA patients included pneumonia and cellulitis.
- Hold treatment with KEVZARA if a patient develops a serious infection or an opportunistic infection.
- Patients with latent TB should be treated with standard antimycobacterial therapy before initiating KEVZARA. Consider anti-TB therapy prior to initiation of KEVZARA in patients with a past history of latent or active TB in whom an adequate course of treatment cannot be confirmed, and for patients with a negative test for latent TB but having risk factors for TB infection.
- Consider the risks and benefits of treatment prior to initiating KEVZARA in patients who have: chronic or recurrent infection, a history of serious or opportunistic infections, underlying conditions that may predispose them to infection, been exposed to TB, or lived in or traveled to areas of endemic TB or endemic mycoses.
- Viral reactivation has been reported with immunosuppressive biologic therapies. Cases of herpes zoster were observed in clinical studies with KEVZARA.
- Laboratory Abnormalities. Treatment with KEVZARA was associated with decreases in absolute neutrophil counts (including neutropenia), and platelet counts; and increases in transaminase levels and lipid parameters (LDL, HDL cholesterol, and/or triglycerides). Increased frequency and magnitude of these elevations were observed when potentially hepatotoxic drugs (e.g., MTX) were used in combination with KEVZARA. Assess neutrophil count, platelet count, and ALT/AST levels prior to initiation with KEVZARA. Monitor these parameters 4 to 8 weeks after start of therapy and every 3 months thereafter. Assess lipid parameters 4 to 8 weeks after start of therapy, then at 6 month intervals.
- Gastrointestinal Perforation. GI perforation risk may be increased with concurrent diverticulitis or concomitant use of NSAIDs or corticosteroids. Gastrointestinal perforations have been reported in clinical studies, primarily as complications of diverticulitis. Promptly evaluate patients presenting with new onset abdominal symptoms.
- Immunosuppression. Treatment with immunosuppressants may result in an increased risk of malignancies. The impact of treatment with KEVZARA on the development of malignancies is not known but malignancies have been reported in clinical studies.
- Hypersensitivity Reactions. Hypersensitivity reactions have been reported in association with KEVZARA. Hypersensitivity reactions that required treatment discontinuation were reported in 0.3% of patients in controlled RA trials. Injection site rash, rash, and urticaria were the most frequent hypersensitivity reactions. Advise patients to seek immediate medical attention if they experience any symptoms of a hypersensitivity reaction. If anaphylaxis or other hypersensitivity reaction occurs, stop administration of KEVZARA immediately. Do not administer KEVZARA to patients with known hypersensitivity to sarilumab.
- Active Hepatic Disease and Hepatic Impairment. Treatment with KEVZARA is not recommended in patients with active hepatic disease or hepatic impairment, as treatment with KEVZARA was associated with transaminase elevations.
- Live Vaccines. Avoid concurrent use of live vaccines during treatment with KEVZARA due to potentially increased risk of infections. No data are available on the secondary transmission of infection from persons receiving live vaccines to patients receiving KEVZARA. Prior to initiating treatment, it is recommended that all patients be brought up to date with all immunizations in agreement with current immunization guidelines.
ADVERSE REACTIONS
- For Rheumatoid Arthritis: The most common serious adverse reactions were infections. The most frequently observed serious infections included pneumonia and cellulitis. The most common adverse reactions (occurred in at least 3% of patients treated with KEVZARA + DMARDs) are neutropenia, increased ALT, injection site erythema, upper respiratory infections, and urinary tract infections.
- For Polymyalgia Rheumatica: Serious adverse reactions of neutropenia occurred in 2 patients (3.4%) in the KEVZARA group compared to none in the placebo group. The proportion of patients with serious infections was similar in the KEVZARA group (5.1%) compared to the placebo group (5.2%). The common adverse reactions occurring in ≥5% of patients treated with KEVZARA were neutropenia, leukopenia, constipation, rash pruritic, myalgia, fatigue, and injection site pruritus.
- For Polyarticular Juvenile Idiopathic Arthritis: In Study 4, the rate of infections was 146.6 events per 100 patient-years. The most common infections observed were nasopharyngitis (36.6%) and upper respiratory tract infections (URTI) (14.0%). The most common adverse drug reactions were nasopharyngitis, neutropenia, upper respiratory tract infection, and injection site erythema.
DRUG INTERACTIONS
- Exercise caution when KEVZARA is co-administered with CYP substrates with a narrow therapeutic index (e.g. warfarin or theophylline), or with CYP3A4 substrates (e.g. oral contraceptives or statins) as there may be a reduction in exposure which may reduce the activity of the CYP3A4 substrate.
- Elevated interleukin-6 (IL-6) concentration may down-regulate CYP activity such as in patients with RA and hence increase drug levels compared to subjects without RA. Blockade of IL-6 signaling by IL-6Rα antagonists such as KEVZARA might reverse the inhibitory effect of IL-6 and restore CYP activity, leading to altered drug concentrations.
USE IN SPECIFIC POPULATIONS
- KEVZARA should be used in pregnancy only if the potential benefit justifies the potential risk to the fetus. Because monoclonal antibodies could be excreted in small amounts in human milk, the benefits of breastfeeding and the potential adverse effects on the breastfed child should be considered along with the mother’s clinical need for KEVZARA.
- Use caution when treating the elderly.
Advise patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Please see full Prescribing Information, including Boxed WARNING.
INDICATIONS
KEVZARA® (sarilumab) is indicated for treatment of:
- adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs (DMARDs).
- adult patients with polymyalgia rheumatica (PMR) who have had an inadequate response to corticosteroids or who cannot tolerate corticosteroid taper.
- patients who weigh 63 kg or greater with active polyarticular juvenile idiopathic arthritis (pJIA).
IMPORTANT SAFETY INFORMATION
|
WARNING: RISK OF SERIOUS INFECTIONS Patients treated with KEVZARA are at increased risk for developing serious infections that may lead to hospitalization or death. Opportunistic infections have also been reported in patients receiving KEVZARA. Most patients who developed infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids. Avoid use of KEVZARA in patients with an active infection. Reported infections include:
Closely monitor patients for signs and symptoms of infection during treatment with KEVZARA. If a serious infection develops, interrupt KEVZARA until the infection is controlled. Consider the risks and benefits of treatment with KEVZARA prior to initiating therapy in patients with chronic or recurrent infection. |
CONTRAINDICATION
Do not use KEVZARA in patients with known hypersensitivity to sarilumab or any of the inactive ingredients.
WARNINGS AND PRECAUTIONS
- Infections. Serious and sometimes fatal infections due to bacterial, mycobacterial, invasive fungal, viral, or other opportunistic pathogens have been reported in patients receiving immunosuppressive agents including KEVZARA. Among opportunistic infections, TB, candidiasis, and pneumocystis were reported with KEVZARA. The most frequently observed serious infections with KEVZARA in RA patients included pneumonia and cellulitis.
- Hold treatment with KEVZARA if a patient develops a serious infection or an opportunistic infection.
- Patients with latent TB should be treated with standard antimycobacterial therapy before initiating KEVZARA. Consider anti-TB therapy prior to initiation of KEVZARA in patients with a past history of latent or active TB in whom an adequate course of treatment cannot be confirmed, and for patients with a negative test for latent TB but having risk factors for TB infection.
- Consider the risks and benefits of treatment prior to initiating KEVZARA in patients who have: chronic or recurrent infection, a history of serious or opportunistic infections, underlying conditions that may predispose them to infection, been exposed to TB, or lived in or traveled to areas of endemic TB or endemic mycoses.
- Viral reactivation has been reported with immunosuppressive biologic therapies. Cases of herpes zoster were observed in clinical studies with KEVZARA.
- Laboratory Abnormalities. Treatment with KEVZARA was associated with decreases in absolute neutrophil counts (including neutropenia), and platelet counts; and increases in transaminase levels and lipid parameters (LDL, HDL cholesterol, and/or triglycerides). Increased frequency and magnitude of these elevations were observed when potentially hepatotoxic drugs (e.g., MTX) were used in combination with KEVZARA. Assess neutrophil count, platelet count, and ALT/AST levels prior to initiation with KEVZARA. Monitor these parameters 4 to 8 weeks after start of therapy and every 3 months thereafter. Assess lipid parameters 4 to 8 weeks after start of therapy, then at 6 month intervals.
- Gastrointestinal Perforation. GI perforation risk may be increased with concurrent diverticulitis or concomitant use of NSAIDs or corticosteroids. Gastrointestinal perforations have been reported in clinical studies, primarily as complications of diverticulitis. Promptly evaluate patients presenting with new onset abdominal symptoms.
- Immunosuppression. Treatment with immunosuppressants may result in an increased risk of malignancies. The impact of treatment with KEVZARA on the development of malignancies is not known but malignancies have been reported in clinical studies.
- Hypersensitivity Reactions. Hypersensitivity reactions have been reported in association with KEVZARA. Hypersensitivity reactions that required treatment discontinuation were reported in 0.3% of patients in controlled RA trials. Injection site rash, rash, and urticaria were the most frequent hypersensitivity reactions. Advise patients to seek immediate medical attention if they experience any symptoms of a hypersensitivity reaction. If anaphylaxis or other hypersensitivity reaction occurs, stop administration of KEVZARA immediately. Do not administer KEVZARA to patients with known hypersensitivity to sarilumab.
- Active Hepatic Disease and Hepatic Impairment. Treatment with KEVZARA is not recommended in patients with active hepatic disease or hepatic impairment, as treatment with KEVZARA was associated with transaminase elevations.
- Live Vaccines. Avoid concurrent use of live vaccines during treatment with KEVZARA due to potentially increased risk of infections. No data are available on the secondary transmission of infection from persons receiving live vaccines to patients receiving KEVZARA. Prior to initiating treatment, it is recommended that all patients be brought up to date with all immunizations in agreement with current immunization guidelines.
ADVERSE REACTIONS
- For Rheumatoid Arthritis: The most common serious adverse reactions were infections. The most frequently observed serious infections included pneumonia and cellulitis. The most common adverse reactions (occurred in at least 3% of patients treated with KEVZARA + DMARDs) are neutropenia, increased ALT, injection site erythema, upper respiratory infections, and urinary tract infections.
- For Polymyalgia Rheumatica: Serious adverse reactions of neutropenia occurred in 2 patients (3.4%) in the KEVZARA group compared to none in the placebo group. The proportion of patients with serious infections was similar in the KEVZARA group (5.1%) compared to the placebo group (5.2%). The common adverse reactions occurring in ≥5% of patients treated with KEVZARA were neutropenia, leukopenia, constipation, rash pruritic, myalgia, fatigue, and injection site pruritus.
- For Polyarticular Juvenile Idiopathic Arthritis: In Study 4, the rate of infections was 146.6 events per 100 patient-years. The most common infections observed were nasopharyngitis (36.6%) and upper respiratory tract infections (URTI) (14.0%). The most common adverse drug reactions were nasopharyngitis, neutropenia, upper respiratory tract infection, and injection site erythema.
DRUG INTERACTIONS
- Exercise caution when KEVZARA is co-administered with CYP substrates with a narrow therapeutic index (e.g. warfarin or theophylline), or with CYP3A4 substrates (e.g. oral contraceptives or statins) as there may be a reduction in exposure which may reduce the activity of the CYP3A4 substrate.
- Elevated interleukin-6 (IL-6) concentration may down-regulate CYP activity such as in patients with RA and hence increase drug levels compared to subjects without RA. Blockade of IL-6 signaling by IL-6Rα antagonists such as KEVZARA might reverse the inhibitory effect of IL-6 and restore CYP activity, leading to altered drug concentrations.
USE IN SPECIFIC POPULATIONS
- KEVZARA should be used in pregnancy only if the potential benefit justifies the potential risk to the fetus. Because monoclonal antibodies could be excreted in small amounts in human milk, the benefits of breastfeeding and the potential adverse effects on the breastfed child should be considered along with the mother’s clinical need for KEVZARA.
- Use caution when treating the elderly.
Advise patients to read the FDA-approved patient labeling (Medication Guide and Instructions for Use).
Please see full Prescribing Information, including Boxed WARNING.
INDICATIONS
KEVZARA® (sarilumab) is indicated for treatment of:
- adult patients with moderately to severely active rheumatoid arthritis (RA) who have had an inadequate response or intolerance to one or more disease-modifying antirheumatic drugs (DMARDs).
- adult patients with polymyalgia rheumatica (PMR) who have had an inadequate response to corticosteroids or who cannot tolerate corticosteroid taper.
- patients who weigh 63 kg or greater with active polyarticular juvenile idiopathic arthritis (pJIA).
Last Updated: May 2026